Does Pulling Out Your Baby Teeth Effect How Your Adult Teeth Come in
| Teeth | |
|---|---|
 Image showing incisors and canine teeth, situated in gums above and below. | |
 Diagram of a human molar showing its major constituents | |
| Details | |
| Identifiers | |
| Latin | dentes |
| TA98 | A05.one.03.001 |
| TA2 | 2818 |
| FMA | 75150 |
| Anatomical terminology [edit on Wikidata] | |
The human teeth part to mechanically break down items of food by cutting and crushing them in preparation for swallowing and digesting. Humans have four types of teeth: incisors, canines, premolars, and molars, which each have a specific part. The incisors cut the nutrient, the canines tear the food and the molars and premolars trounce the food. The roots of teeth are embedded in the maxilla (upper jaw) or the mandible (lower jaw) and are covered by gums. Teeth are made of multiple tissues of varying density and hardness.
Humans, like nigh other mammals, are diphyodont, significant that they develop two sets of teeth. The first set, deciduous teeth, also called "primary teeth", "baby teeth", or "milk teeth", unremarkably somewhen contains xx teeth. Main teeth typically start to appear ("erupt") around six months of age and this may exist distracting and/or painful for the babe. Even so, some babies are built-in with one or more visible teeth, known every bit neonatal teeth or "natal teeth".
Anatomy
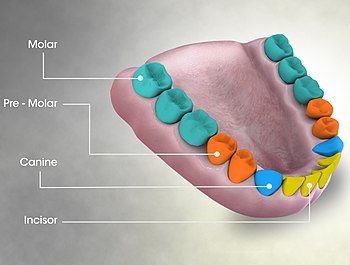
There are four primary types of teeth in humans, shown labelled here.
Dental anatomy is a field of beefcake dedicated to the study of tooth structure. The development, appearance, and classification of teeth fall within its field of study, though dental occlusion, or contact betwixt teeth, does not. Dental beefcake is also a taxonomic science as information technology is concerned with the naming of teeth and their structures. This information serves a practical purpose for dentists, enabling them to easily place and describe teeth and structures during treatment.
The anatomic crown of a tooth is the expanse covered in enamel higher up the cementoenamel junction (CEJ) or "neck" of the tooth.[1] [2] Most of the crown is equanimous of dentin ("dentine" in British English) with the pulp bedroom within.[3] The crown is within bone earlier eruption.[4] Afterwards eruption, it is almost ever visible. The anatomic root is plant beneath the CEJ and is covered with cementum. As with the crown, dentin composes most of the root, which normally has lurid canals. Canines and almost premolars, except for maxillary first premolars, ordinarily have 1 root. Maxillary start premolars and mandibular molars usually have 2 roots. Maxillary molars usually accept three roots. Boosted roots are referred to as supernumerary roots.
Humans usually have xx master (deciduous, "baby" or "milk") teeth and 32 permanent (adult) teeth. Teeth are classified as incisors, canines, premolars (as well called bicuspids), and molars. Incisors are primarily used for cutting, canines are for tearing, and molars serve for grinding.
Most teeth take identifiable features that distinguish them from others. There are several dissimilar notation systems to refer to a specific tooth. The 3 most common systems are the FDI World Dental Federation notation (ISO 3950), the Universal Numbering System, and the Palmer notation. The FDI organization is used worldwide, the Universal only in the United States, while the older Palmer annotation still has some adherents but in the United Kingdom.
Primary teeth
Among deciduous (primary) teeth, 10 are found in the maxilla (upper jaw) and ten in the mandible (lower jaw), for a total of 20. The dental formula for primary teeth in humans is ii.i.0.ii 2.1.0.2 .
In the main set of teeth, there are ii types of incisors—centrals and laterals—and two types of molars—get-go and 2d. All chief teeth are normally later on replaced with their permanent counterparts.
Permanent teeth

The Universal Numbering System for adult human teeth. The view is from a dental practitioner'southward perspective, meaning tooth 1 is the upper right rear (tertiary) molar.
Among permanent teeth, 16 are found in the maxilla and 16 in the mandible, for a total of 32. The dental formula is 2.1.2.3 2.ane.2.three . Permanent homo teeth are numbered in a boustrophedonic sequence.
The maxillary teeth are the maxillary central incisors (teeth 8 and 9 in the diagram), maxillary lateral incisors (7 and 10), maxillary canines (six and 11), maxillary first premolars (5 and 12), maxillary 2nd premolars (4 and 13), maxillary first molars (iii and fourteen), maxillary second molars (ii and 15), and maxillary 3rd molars (1 and xvi). The mandibular teeth are the mandibular central incisors (24 and 25), mandibular lateral incisors (23 and 26), mandibular canines (22 and 27), mandibular first premolars (21 and 28), mandibular second premolars (twenty and 29), mandibular first molars (19 and 30), mandibular 2d molars (18 and 31), and mandibular third molars (17 and 32). Third molars are commonly chosen "wisdom teeth" usually emerge at ages 17 to 25.[5] These molars may never erupt into the mouth or form at all[ commendation needed ]. When they do form, they often must be removed. If any additional teeth class—for example, fourth and fifth molars, which are rare—they are referred to as supernumerary teeth (hyperdontia). Development of fewer than the usual number of teeth is called hypodontia.
In that location are small differences betwixt the teeth of males and females, with male teeth along with the male jaw disposed to be larger on average than female person teeth and jaw. There are as well differences in the internal dental tissue proportions, with male person teeth consisting of proportionately more dentine while female teeth have proportionately more enamel.[6]
Parts

Enamel
Enamel is the hardest and nigh highly mineralized substance of the body. It has its origin from oral ectoderm. It is 1 of the 4 major tissues which make up the tooth, along with dentin, cementum, and dental lurid.[7] It is normally visible and must be supported past underlying dentin. 96% of enamel consists of mineral, with water and organic textile comprising the residuum.[8] The normal color of enamel varies from lite yellow to grayish white. At the edges of teeth where at that place is no dentin underlying the enamel, the color sometimes has a slightly bluish tone. Since enamel is semitranslucent, the color of dentin and any restorative dental cloth underneath the enamel strongly affects the advent of a tooth. Enamel varies in thickness over the surface of the tooth and is often thickest at the cusp, upwards to ii.5mm, and thinnest at its border, which is seen clinically as the CEJ.[9] The wearable charge per unit of enamel, called compunction, is viii micrometers a twelvemonth from normal factors.[ten]
Enamel'due south main mineral is hydroxyapatite, which is a crystalline calcium phosphate.[11] The large amount of minerals in enamel accounts non only for its strength but as well for its brittleness.[9] Dentin, which is less mineralized and less brittle, compensates for enamel and is necessary as a support.[11] Unlike dentin and bone, enamel does not contain collagen. Proteins of notation in the evolution of enamel are ameloblastins, amelogenins, enamelins and tuftelins. It is believed that they aid in the development of enamel by serving equally framework back up, among other functions.[12] In rare circumstances enamel tin neglect to grade, leaving the underlying dentine exposed on the surface.[13]
Dentin
Dentin is the substance between enamel or cementum and the pulp chamber. It is secreted by the odontoblasts of the dental pulp.[14] The formation of dentin is known as dentinogenesis. The porous, yellow-hued material is made up of 70% inorganic materials, twenty% organic materials, and 10% water by weight.[15] Considering it is softer than enamel, it decays more than rapidly and is subject area to astringent cavities if not properly treated, merely dentin still acts as a protective layer and supports the crown of the tooth.
Dentin is a mineralized connective tissue with an organic matrix of collagenous proteins. Dentin has microscopic channels, called dentinal tubules, which radiate outward through the dentin from the pulp cavity to the exterior cementum or enamel border.[xvi] The diameter of these tubules range from 2.5 μm almost the lurid, to one.2 μm in the midportion, and 900 nm well-nigh the dentino-enamel junction.[17] Although they may accept tiny side-branches, the tubules exercise not intersect with each other. Their length is dictated past the radius of the molar. The 3 dimensional configuration of the dentinal tubules is genetically determined.
At that place are iii types of dentin, primary, secondary and third.[18] Secondary dentin is a layer of dentin produced afterwards root formation and continues to form with age. Third dentin is created in response to stimulus, such as cavities and tooth wear.[xix]
Cementum
Cementum is a specialized bone similar substance covering the root of a molar.[14] Information technology is approximately 45% inorganic textile (mainly hydroxyapatite), 33% organic fabric (mainly collagen) and 22% water. Cementum is excreted by cementoblasts within the root of the tooth and is thickest at the root apex. Its coloration is yellowish and it is softer than dentin and enamel. The principal function of cementum is to serve as a medium by which the periodontal ligaments tin can attach to the molar for stability. At the cement to enamel junction, the cementum is acellular due to its lack of cellular components, and this acellular type covers at least ⅔ of the root.[20] The more permeable form of cementum, cellular cementum, covers about ⅓ of the root apex.[21]
Dental pulp
The dental pulp is the central part of the tooth filled with soft connective tissue.[15] This tissue contains claret vessels and nerves that enter the tooth from a pigsty at the apex of the root.[22] Forth the edge betwixt the dentin and the pulp are odontoblasts, which initiate the formation of dentin.[xv] Other cells in the pulp include fibroblasts, preodontoblasts, macrophages and T lymphocytes.[23] The pulp is commonly called "the nerve" of the tooth.
Development

Radiograph of lower right third, 2d, and first molars in different stages of evolution
Tooth evolution is the complex process by which teeth form from embryonic cells, grow, and erupt into the oral cavity. Although many diverse species have teeth, their development is largely the same every bit in humans. For human teeth to have a healthy oral environment, enamel, dentin, cementum, and the periodontium must all develop during advisable stages of fetal development. Primary teeth kickoff to course in the development of the embryo between the 6th and eighth weeks, and permanent teeth begin to form in the twentieth week.[24] If teeth do not kickoff to develop at or near these times, they volition not develop at all.
A significant corporeality of research has focused on determining the processes that initiate tooth development. It is widely accepted that there is a factor within the tissues of the first pharyngeal curvation that is necessary for the development of teeth.[25]
Tooth development is usually divided into the following stages: the bud phase, the cap, the bell, and finally maturation. The staging of tooth development is an attempt to categorize changes that accept identify along a continuum; frequently information technology is hard to decide what phase should be assigned to a item developing tooth.[25] This determination is further complicated by the varying appearance of different histologic sections of the same developing tooth, which can appear to exist different stages.
The tooth bud (sometimes called the molar germ) is an aggregation of cells that eventually forms a tooth. Information technology is organized into three parts: the enamel organ, the dental papilla and the dental follicle.[26] The enamel organ is equanimous of the outer enamel epithelium, inner enamel epithelium, stellate reticulum and stratum intermedium.[26] These cells give ascension to ameloblasts, which produce enamel and the reduced enamel epithelium. The growth of cervical loop cells into the deeper tissues forms Hertwig'southward Epithelial Root Sheath, which determines a tooth'south root shape. The dental papilla contains cells that develop into odontoblasts, which are dentin-forming cells.[26] Additionally, the junction between the dental papilla and inner enamel epithelium determines the crown shape of a molar.[27] The dental follicle gives rising to three important cells: cementoblasts, osteoblasts, and fibroblasts. Cementoblasts form the cementum of a tooth. Osteoblasts give rise to the alveolar bone effectually the roots of teeth. Fibroblasts develop the periodontal ligaments which connect teeth to the alveolar bone through cementum.[28]
Eruption

Bottom teeth of a seven-twelvemonth-old, showing chief teeth (left), a lost primary tooth (middle), and a permanent tooth (right)
Molar eruption in humans is a procedure in tooth development in which the teeth enter the mouth and go visible. Current research indicates that the periodontal ligaments play an of import part in tooth eruption. Primary teeth erupt into the mouth from around six months until two years of age. These teeth are the but ones in the mouth until a person is well-nigh six years old. At that time, the first permanent tooth erupts. This stage, during which a person has a combination of principal and permanent teeth, is known as the mixed stage. The mixed stage lasts until the terminal main tooth is lost and the remaining permanent teeth erupt into the mouth.
There have been many theories about the crusade of tooth eruption. 1 theory proposes that the developing root of a molar pushes it into the mouth. Another, known every bit the cushioned hammock theory, resulted from microscopic study of teeth, which was idea to testify a ligament around the root. It was afterward discovered that the "ligament" was merely an artifact created in the process of preparing the slide. Currently, the nearly widely held conventionalities is that the periodontal ligaments provide the main impetus for the process.
The onset of master molar loss has been constitute to correlate strongly with somatic and psychological criteria of school readiness.[29] [30] [ clarification needed ]
Supporting structures

Histologic slide of tooth erupting into the rima oris
A: tooth
B: gingiva
C: bone
D: periodontal ligaments
The periodontium is the supporting structure of a molar, helping to attach the tooth to surrounding tissues and to allow sensations of touch and pressure.[31] It consists of the cementum, periodontal ligaments, alveolar os, and gingiva. Of these, cementum is the only one that is a part of a tooth. Periodontal ligaments connect the alveolar bone to the cementum. Alveolar os surrounds the roots of teeth to provide support and creates what is ordinarily called an air sac, or "socket". Lying over the bone is the gingiva or gum, which is readily visible in the oral fissure.
Periodontal ligaments
The periodontal ligament is a specialized connective tissue that attaches the cementum of a tooth to the alveolar bone. This tissue covers the root of the molar within the bone. Each ligament has a width of 0.15–0.38mm, but this size decreases over time.[32] The functions of the periodontal ligaments include zipper of the tooth to the bone, support for the molar, germination and resorption of bone during tooth move, sensation, and eruption.[28] The cells of the periodontal ligaments include osteoblasts, osteoclasts, fibroblasts, macrophages, cementoblasts, and epithelial prison cell rests of Malassez.[33] Consisting of mostly Type I and Iii collagen, the fibers are grouped in bundles and named according to their location. The groups of fibers are named alveolar crest, horizontal, oblique, periapical, and interradicular fibers.[34] The nerve supply generally enters from the bone upmost to the tooth and forms a network effectually the tooth toward the crest of the gingiva.[35] When pressure level is exerted on a tooth, such as during chewing or biting, the tooth moves slightly in its socket and puts tension on the periodontal ligaments. The nerve fibers tin then send the information to the central nervous system for interpretation.
Alveolar os
The alveolar os is the os of the jaw which forms the air sac around teeth.[36] Like whatsoever other os in the man body, alveolar os is modified throughout life. Osteoblasts create bone and osteoclasts destroy information technology, especially if force is placed on a molar.[31] As is the instance when movement of teeth is attempted through orthodontics, an surface area of os under compressive force from a molar moving toward it has a loftier osteoclast level, resulting in bone resorption. An area of os receiving tension from periodontal ligaments attached to a molar moving abroad from it has a high number of osteoblasts, resulting in os formation.
Gingiva
The gingiva ("gums") is the mucosal tissue that overlays the jaws. There are 3 different types of epithelium associated with the gingiva: gingival, junctional, and sulcular epithelium. These three types form from a mass of epithelial cells known every bit the epithelial cuff between the tooth and the mouth.[37] The gingival epithelium is not associated directly with tooth attachment and is visible in the mouth. The junctional epithelium, composed of the basal lamina and hemidesmosomes, forms an attachment to the tooth.[28] The sulcular epithelium is nonkeratinized stratified squamous tissue on the gingiva which touches only is not attached to the tooth.[38]
Tooth decay
Plaque
Plaque is a biofilm consisting of large quantities of various bacteria that course on teeth.[39] If not removed regularly, plaque buildup can lead to periodontal issues such as gingivitis. Given time, plaque tin can mineralize along the gingiva, forming tartar. The microorganisms that grade the biofilm are most entirely leaner (mainly streptococcus and anaerobes), with the composition varying by location in the mouth.[40] Streptococcus mutans is the near important bacterium associated with dental caries.
Certain bacteria in the oral cavity alive off the remains of foods, especially sugars and starches. In the absence of oxygen they produce lactic acid, which dissolves the calcium and phosphorus in the enamel.[14] [41] This process, known as "demineralisation", leads to tooth destruction. Saliva gradually neutralises the acids which crusade the pH of the tooth surface to rise above the critical pH, typically considered to exist 5.v. This causes 'remineralisation', the return of the dissolved minerals to the enamel. If there is sufficient time between the intake of foods so the affect is limited and the teeth can repair themselves. Saliva is unable to penetrate through plaque, however, to neutralize the acid produced by the bacteria.
Caries (cavities)

Advanced tooth decay on a premolar
Dental caries (cavities), described every bit "tooth decay", is an infectious disease which damages the structures of teeth.[42] The disease can atomic number 82 to pain, tooth loss, and infection. Dental caries has a long history, with evidence showing the disease was nowadays in the Bronze, Iron, and Middle ages just too prior to the neolithic menses.[43] The largest increases in the prevalence of caries take been associated with diet changes.[44] Today, caries remains one of the virtually common diseases throughout the world. In the United States, dental caries is the most common chronic babyhood illness, existence at least v times more than common than asthma.[45] Countries that accept experienced an overall decrease in cases of tooth decay go on to take a disparity in the distribution of the disease.[46] Amongst children in the United states and Europe, 60–80% of cases of dental caries occur in 20% of the population.[47]
Tooth decay is caused by sure types of acid-producing leaner which cause the most damage in the presence of fermentable carbohydrates such as sucrose, fructose, and glucose.[48] [49] The resulting acidic levels in the mouth bear on teeth considering a molar's special mineral content causes it to be sensitive to low pH. Depending on the extent of molar destruction, various treatments can be used to restore teeth to proper form, function, and aesthetics, just at that place is no known method to regenerate large amounts of tooth structure. Instead, dental health organizations advocate preventive and prophylactic measures, such equally regular oral hygiene and dietary modifications, to avoid dental caries.[l]
Tooth care
Oral hygiene

Oral hygiene is the practice of keeping the oral fissure clean and is a ways of preventing dental caries, gingivitis, periodontal disease, bad breath, and other dental disorders. It consists of both professional and personal intendance. Regular cleanings, usually done by dentists and dental hygienists, remove tartar (mineralized plaque) that may develop fifty-fifty with careful brushing and flossing. Professional cleaning includes tooth scaling, using diverse instruments or devices to loosen and remove deposits from teeth.
The purpose of cleaning teeth is to remove plaque, which consists generally of bacteria.[51] Healthcare professionals recommend regular brushing twice a day (in the morning and in the evening, or after meals) in gild to prevent germination of plaque and tartar.[50] A toothbrush is able to remove most plaque, except in areas between teeth. As a result, flossing is besides considered a necessity to maintain oral hygiene. When used correctly, dental floss removes plaque from between teeth and at the mucilage line, where periodontal illness ofttimes begins and could develop caries.
Electric toothbrushes are a pop help to oral hygiene. A user without disabilities, with proper preparation in manual brushing, and with skillful motivation, tin can achieve standards of oral hygiene at to the lowest degree as satisfactory equally the best electric brushes, merely untrained users rarely accomplish anything of the kind. Not all electrical toothbrushes are equally effective and even a good design needs to exist used properly for best effect, but: "Electrical toothbrushes tend to help people who are not every bit skilful at cleaning teeth and as a result accept had oral hygiene issues."[52] The most important reward of electric toothbrushes is their ability to aid people with dexterity difficulties, such as those associated with rheumatoid arthritis.
Protective treatments
Fluoride therapy is often recommended to protect against dental caries. Water fluoridation and fluoride supplements decrease the incidence of dental caries. Fluoride helps prevent dental decay by binding to the hydroxyapatite crystals in enamel.[53] The incorporated fluoride makes enamel more resistant to demineralization and thus more resistant to decay.[28] Topical fluoride, such equally a fluoride toothpaste or mouthwash, is also recommended to protect teeth surfaces. Many dentists include application of topical fluoride solutions as part of routine cleanings.
Dental sealants are another preventive therapy ofttimes used to provide a barrier to bacteria and decay on the surface of teeth. Sealants can last upwards to 10 years and are primarily used on the biting surfaces of molars of children and young adults, particularly those who may have difficulty brushing and flossing effectively. Sealants are applied in a dentist'south office, sometimes by a dental hygienist, in a procedure similar in technique and cost to a fluoride application.
Restorations

Afterward a tooth has been damaged or destroyed, restoration of the missing structure can be achieved with a diversity of treatments. Restorations may be created from a multifariousness of materials, including glass ionomer, constructing, gold, porcelain, and composite.[54] Minor restorations placed inside a tooth are referred to as "intracoronal restorations". These restorations may exist formed directly in the oral cavity or may exist cast using the lost-wax technique, such as for some inlays and onlays. When larger portions of a tooth are lost, an "extracoronal restoration" may be fabricated, such as an artificial crown or a veneer, to restore the involved tooth.
When a tooth is lost, dentures, bridges, or implants may be used equally replacements.[55] Dentures are commonly the least costly whereas implants are commonly the most expensive. Dentures may replace complete arches of the mouth or only a partial number of teeth. Bridges replace smaller spaces of missing teeth and use side by side teeth to support the restoration. Dental implants may exist used to replace a single tooth or a series of teeth. Though implants are the virtually expensive treatment selection, they are often the most desirable restoration because of their aesthetics and office. To amend the function of dentures, implants may be used as support.[56]
Abnormalities

A broken upper front molar showing the pink of the lurid
Tooth abnormalities may be categorized according to whether they have environmental or developmental causes.[57] While environmental abnormalities may appear to have an obvious cause, there may non appear to be any known cause for some developmental abnormalities. Environmental forces may affect teeth during development, destroy molar construction after development, discolor teeth at any stage of evolution, or alter the form of tooth eruption. Developmental abnormalities nigh ordinarily touch on the number, size, shape, and structure of teeth.
Ecology
Alteration during tooth development
Molar abnormalities caused past environmental factors during tooth development take long-lasting effects. Enamel and dentin practice not regenerate after they mineralize initially. Enamel hypoplasia is a condition in which the amount of enamel formed is inadequate.[58] This results either in pits and grooves in areas of the tooth or in widespread absence of enamel. Diffuse opacities of enamel does not affect the amount of enamel but changes its appearance. Affected enamel has a different translucency than the balance of the tooth. Demarcated opacities of enamel have sharp boundaries where the translucency decreases and manifest a white, foam, yellow, or brown color. All these may be caused by nutritional factors,[59] an exanthematous disease (chicken pox, congenital syphilis),[59] [60] undiagnosed and untreated celiac affliction,[61] [62] [63] hypocalcemia, dental fluorosis, birth injury, preterm nascence, infection or trauma from a deciduous tooth.[59] Dental fluorosis is a condition which results from ingesting excessive amounts of fluoride and leads to teeth which are spotted, yellow, brown, black or sometimes pitted. In about cases, the enamel defects caused past celiac illness, which may exist the merely manifestation of this disease in the absence of any other symptoms or signs, are not recognized and mistakenly attributed to other causes, such equally fluorosis.[61] Enamel hypoplasia resulting from syphilis is frequently referred to as Hutchinson's teeth, which is considered one role of Hutchinson'due south triad.[64] Turner's hypoplasia is a portion of missing or diminished enamel on a permanent molar usually from a prior infection of a nearby chief tooth. Hypoplasia may likewise result from antineoplastic therapy.
Destruction subsequently evolution
Tooth destruction from processes other than dental caries is considered a normal physiologic process just may become severe plenty to become a pathologic condition. Compunction is the loss of tooth structure past mechanical forces from opposing teeth.[65] Attrition initially affects the enamel and, if unchecked, may proceed to the underlying dentin. Abrasion is the loss of tooth structure by mechanical forces from a foreign element.[66] If this forcefulness begins at the cementoenamel junction, then progression of tooth loss can be rapid since enamel is very thin in this region of the tooth. A mutual source of this blazon of tooth wearable is excessive force when using a toothbrush. Erosion is the loss of molar structure due to chemical dissolution past acids non of bacterial origin.[67] Signs of molar destruction from erosion is a mutual feature in the mouths of people with bulimia since airsickness results in exposure of the teeth to gastric acids. Another important source of erosive acids are from frequent sucking of lemon juice. Abfraction is the loss of tooth structure from flexural forces. Every bit teeth flex under pressure, the arrangement of teeth touching each other, known every bit occlusion, causes tension on one side of the tooth and compression on the other side of the tooth. This is believed to crusade Five-shaped depressions on the side under tension and C-shaped depressions on the side under compression. When tooth destruction occurs at the roots of teeth, the procedure is referred to as internal resorption, when caused by cells within the pulp, or external resorption, when caused past cells in the periodontal ligament.
Discoloration

Discoloration of teeth may result from bacteria stains, tobacco, tea, java, foods with an abundance of chlorophyll, restorative materials, and medications.[68] Stains from bacteria may cause colors varying from greenish to blackness to orange. Dark-green stains likewise result from foods with chlorophyll or excessive exposure to copper or nickel. Amalgam, a common dental restorative textile, may turn adjacent areas of teeth blackness or gray. Long term use of chlorhexidine, a mouthwash, may encourage extrinsic stain formation near the gingiva on teeth. This is usually easy for a hygienist to remove. Systemic disorders too tin can crusade molar discoloration. Congenital erythropoietic porphyria causes porphyrins to be deposited in teeth, causing a carmine-brownish coloration. Blue discoloration may occur with alkaptonuria and rarely with Parkinson's illness. Erythroblastosis fetalis and biliary atresia are diseases which may cause teeth to announced green from the deposition of biliverdin. Too, trauma may change a molar to a pink, yellowish, or night grayness color. Pink and red discolorations are too associated in patients with lepromatous leprosy. Some medications, such as tetracycline antibiotics, may become incorporated into the construction of a tooth, causing intrinsic staining of the teeth.
Alteration of eruption
Tooth eruption may exist altered by some environmental factors. When eruption is prematurely stopped, the tooth is said to be impacted. The most common cause of tooth impaction is lack of space in the oral cavity for the tooth.[69] Other causes may exist tumors, cysts, trauma, and thickened bone or soft tissue. Tooth ankylosis occurs when the tooth has already erupted into the oral fissure only the cementum or dentin has fused with the alveolar bone. This may cause a person to retain their primary molar instead of having information technology replaced by a permanent one.
A technique for altering the natural progression of eruption is employed by orthodontists who wish to filibuster or speed up the eruption of certain teeth for reasons of infinite maintenance or otherwise preventing crowding and/or spacing. If a principal tooth is extracted before its succeeding permanent tooth's root reaches ⅓ of its total growth, the eruption of the permanent tooth will exist delayed. Conversely, if the roots of the permanent tooth are more than ⅔ complete, the eruption of the permanent tooth will be accelerated. Between ⅓ and ⅔, it is unknown exactly what will occur to the speed of eruption.
Developmental
Abnormality in number
- Anodontia is the total lack of tooth development.
- Hyperdontia is the presence of a higher-than-normal number of teeth.
- Hypodontia is the lack of development of ane or more teeth.
- Oligodontia may exist used to describe the absenteeism of 6 or more teeth.
Some systemic disorders which may result in hyperdontia include Apert syndrome, cleidocranial dysostosis, Crouzon syndrome, Ehlers–Danlos syndrome, Gardner's syndrome, and Sturge–Weber syndrome.[70] Some systemic disorders which may upshot in hypodontia include Crouzon syndrome, Ectodermal dysplasia, Ehlers–Danlos syndrome, and Gorlin syndrome.[71]
Abnormality in size
- Microdontia is a condition where teeth are smaller than the usual size.
- Macrodontia is where teeth are larger than the usual size.
Microdontia of a unmarried tooth is more than likely to occur in a maxillary lateral incisor. The second most likely tooth to have microdontia are third molars. Macrodontia of all the teeth is known to occur in pituitary gigantism and pineal hyperplasia. Information technology may also occur on one side of the confront in cases of hemifacial hyperplasia.
Abnormality in shape

The fusion of two deciduous teeth
- Gemination occurs when a developing tooth incompletely splits into the formation of two teeth.
- Fusion is the marriage of 2 side by side teeth during development.
- Concrescence is the fusion of two separate teeth only in their cementum.
- Accessory cusps are additional cusps on a molar and may manifest as a Talon cusp, Cusp of Carabelli, or Dens evaginatus.
- Dens invaginatus, likewise called Dens in dente, is a deep invagination in a molar causing the advent of a tooth within a tooth.
- Ectopic enamel is enamel found in an unusual location, such as the root of a tooth.
- Taurodontism is a condition where the body of the tooth and lurid bedchamber is enlarged, and is associated with Klinefelter syndrome, Tricho-dento-osseous syndrome, Triple X syndrome, and XYY syndrome.[72]
- Hypercementosis is excessive formation of cementum, which may effect from trauma, inflammation, acromegaly, rheumatic fever, and Paget's affliction of os.[72]
- A dilaceration is a bend in the root which may accept been caused by trauma to the tooth during germination.
- Supernumerary roots is the presence of a greater number of roots on a tooth than expected
Cleft lip and palate and their association with dental anomalies
There are many types of dental anomalies seen in crevice lip and palate (CLP) patients. Both sets of dentition may be affected; nevertheless, they are normally seen in the afflicted side. Almost frequently, missing teeth, supernumerary or discoloured teeth can be seen; however, enamel dysplasia, discolouration and delayed root evolution are also common. In children with cleft lip and palate, the lateral incisor in the alveolar cleft region has the highest prevalence of dental developmental disorders;[73] this condition may be a cause of tooth crowding.[74] This is important to consider in guild to correctly plan treatment keeping in mind considerations for role and aesthetics. By correctly coordinating management invasive treatment procedures tin be prevented resulting in successful and bourgeois treatment.
In that location have been a plethora of inquiry studies to summate prevalence of certain dental anomalies in CLP populations nonetheless a variety of results have been obtained.
In a report evaluating dental anomalies in Brazilian crevice patients, male person patients had a higher incidence of CLP, agenesis, and supernumerary teeth than did female person patients. In cases of complete CLP, the left maxillary lateral incisor was the most commonly absent molar. Supernumerary teeth were typically located distal to the crevice.[75] In a study of Jordanian subjects, the prevalence of dental anomaly was higher in CLP patients than in normal subjects. Missing teeth were observed in 66.7% of patients, with maxillary lateral incisor equally the most frequently afflicted tooth. Supernumerary teeth were observed in xvi.seven% of patients; other findings included microdontia (37%), taurodontism (70.5%), transposition or ectopic teeth (xxx.8%), dilacerations (19.two%), and hypoplasia (thirty.8%). The incidence of microdontia, dilaceration, and hypoplasia was significantly higher in bilateral CLP patients than in unilateral CLP patients, and none of the anomalies showed any pregnant sexual dimorphism.[76]
Information technology is therefore evident that patients with cleft lip and palate may present with a variety of dental anomalies. It is essential to appraise the patient both clinically and radiographically in order to correctly treat and prevent progression of any dental issues. It is besides useful to note that patients with a cleft lip and palate automatically score a 5 on the IOTN ( index for orthodontic need) and therefore are eligible for orthodontic handling, liaising with an orthodontist is vital in social club coordinate and plan handling successfully.
Abnormality in structure
- Amelogenesis imperfecta is a condition in which enamel does not form properly or at all.[77]
- Dentinogenesis imperfecta is a condition in which dentin does not course properly and is sometimes associated with osteogenesis imperfecta.[78]
- Dentin dysplasia is a disorder in which the roots and pulp of teeth may exist afflicted.
- Regional odontodysplasia is a disorder affecting enamel, dentin, and lurid and causes the teeth to appear "ghostly" on radiographs.[79]
- Diastema is a condition in which there is a gap between two teeth caused by the imbalance in the relationship betwixt the jaw and the size of teeth.[80]
See also
- Barodontalgia
- Dentistry
- Dental auxiliary
- Dental assistant
- Dental hygienist
- Dental technician
- Dental braces
- Dental notation
- Dental tourism
- Caput and cervix anatomy
- Regenerative endodontics
- Socket preservation
- Natural language
- Tooth fairy
- Molar painting
- Tooth regeneration
Lists
- List of bones dentistry topics
- List of oral health and dental topics
References
Notes
- ^ Clemente, Carmine (1987). Anatomy, a regional atlas of the human being body. Baltimore: Urban & Schwarzenberg. ISBN978-0-8067-0323-seven.
- ^ Ash 2003, p. 6
- ^ Cate 1998, p. 3
- ^ Ash 2003, p. nine
- ^ "Impacted wisdom teeth". Mayo Dispensary. Retrieved 5 March 2022.
- ^ Sorenti, Mark; Martinón‐Torres, María; Martín‐Francés, Laura; Perea‐Pérez, Bernardo (2019). "Sexual dimorphism of dental tissues in modern human mandibular molars". American Periodical of Physical Anthropology. 169 (2): 332–340. doi:10.1002/ajpa.23822. ISSN 1096-8644. PMID 30866041.
- ^ Ross 2002, p. 441
- ^ Cate 1998, p. 1
- ^ a b Cate 1998, p. 219
- ^ "Tooth enamel | Drug Discrimination Database".
- ^ a b Johnson, Clarke (1998). "Biology of the Human Dentition Archived 2015-10-thirty at the Wayback Auto". uic.edu.
- ^ Cate 1998, p. 198
- ^ "Severe Plane-Form Enamel Hypoplasia in a Dentition from Roman Britain". ResearchGate . Retrieved 2019-01-09 .
- ^ a b c Ross 2002, p. 448
- ^ a b c Cate 1998, p. 150
- ^ Ross 2002, p. 450
- ^ Cate 1998, p. 152
- ^ Zilberman, U.; Smith, P. (2001). "Sex- and Age-related Differences in Primary and Secondary Dentin Formation". Advances in Dental Research. 15: 42–45. CiteSeerXten.ane.1.535.5123. doi:10.1177/08959374010150011101. PMID 12640738. S2CID 4798656.
- ^ "Tertiary Dentine Frequencies in Extant Great Apes and Fossil Hominins". ResearchGate . Retrieved 2019-03-28 .
- ^ Cate 1998, p. 236
- ^ Cate 1998, p. 241
- ^ Ross 2002, p. 451
- ^ Walton, Richard Due east. and Mahmoud Torabinejad. Principles and Practice of Endodontics. 3rd ed. 2002. pp. eleven–13. ISBN 0-7216-9160-ix.
- ^ Cate 1998, p. 95
- ^ a b Cate 1998, p. 81
- ^ a b c Lab Exercises: Tooth development. Academy of Texas Medical Branch.
- ^ Cate 1998, pp. 86 and 102.
- ^ a b c d Ross 2002, p. 453
- ^ Kranich, Ernst-Michael (1990) "Anthropologie", in F. Bohnsack and Eastward-M Kranich (eds.), Erziehungswissenschaft und Waldorfpädagogik, Reihe Pädagogik Beltz, Weinheim, p. 126, citing Frances Ilg and Louise Bates Ames (Gesell Institute), School Readiness, p. 236 ff
- ^ Silvestro, JR (1977). "2d Dentition and School Readiness". New York State Dental Journal. 43 (3): 155–viii. PMID 264640.
...the loss of the first deciduous tooth tin can serve as a definite indicator of a male child's readiness for reading and schoolwork
- ^ a b Ross 2002, p. 452
- ^ Cate 1998, p. 256
- ^ Cate 1998, p. 260
- ^ Listgarten, Max A. "Histology of the Periodontium: Principal fibers of the periodontal ligament," University of Pennsylvania and Temple University. Created May eight, 1999, revised xvi January 2007.
- ^ Cate 1998, p. 270
- ^ Cate 1998, p. 274
- ^ Cate 1998, pp. 247 and 248
- ^ Cate 1998, p. 280
- ^ "Oral Wellness Topics: Plaque", American Dental Association.
- ^ Introduction to dental plaque Archived 2011-08-27 at the Wayback Auto, Leeds Dental Institute.
- ^ Ophardt, Charles Due east. "Sugar and molar decay", Elmhurst College.
- ^ Dental Cavities, MedlinePlus Medical Encyclopedia.
- ^ Seiler R, Spielman AI, Zink A, Rühli F (2013). "Oral pathologies of the Neolithic Iceman, c.iii,300 BC". European Journal of Oral Sciences (Historical Commodity. Research Support, Non-U.South. Gov't). 121 (3 Pt i): 137–41. doi:ten.1111/eos.12037. PMID 23659234.
- ^ Suddick RP, Harris NO (1990). "Historical perspectives of oral biology: a series". Crit. Rev. Oral Biol. Med. 1 (2): 135–51. doi:10.1177/10454411900010020301. PMID 2129621.
- ^ Healthy People: 2010. Good for you People.gov.
- ^ "Dental caries", from the Disease Control Priorities Projection.
- ^ Touger-Decker R, van Loveren C (2003). "Sugars and dental caries". Am. J. Clin. Nutr. 78 (4): 881S–892S. doi:10.1093/ajcn/78.4.881S. PMID 14522753.
- ^ Hardie JM (1982). "The microbiology of dental caries". Dent Update. nine (four): 199–200, 202–4, 206–8. PMID 6959931.
- ^ Moore WJ; Moore, West.J. (1983). "The part of sugar in the aetiology of dental caries. 1. Saccharide and the antiquity of dental caries". J Dent. xi (three): 189–ninety. doi:10.1016/0300-5712(83)90182-3. PMID 6358295.
- ^ a b Oral Health Topics: Cleaning your teeth and gums. American Dental Association.
- ^ Introduction to Dental Plaque Archived 2011-08-27 at the Wayback Machine. Leeds Dental Found.
- ^ Thumbs down for electric toothbrush, BBC News, January 21, 2003.
- ^ Cate 1998, p. 223
- ^ "Oral Health Topics: Dental Filling Options". ada.org.
- ^ "Prosthodontic Procedures", The American College of Prosthodontists.
- ^ "Dental Implants", American Association of Oral and Maxillofacial Surgeons.
- ^ Neville 2002, p. l.
- ^ Ash 2003, p. 31
- ^ a b c Kanchan T, Machado K, Rao A, Krishan Thousand, Garg AK (Apr 2015). "Enamel hypoplasia and its role in identification of individuals: A review of literature". Indian J Dent (Revisión). half-dozen (2): 99–102. doi:10.4103/0975-962X.155887. PMC4455163. PMID 26097340.
- ^ Neville 2002, p. 51
- ^ a b Dental Enamel Defects and Celiac Illness Archived 2016-03-05 at the Wayback Machine National Plant of Health (NIH)
- ^ Ferraz EG, Campos Ede J, Sarmento VA, Silva LR (2012). "The oral manifestations of celiac disease: information for the pediatric dentist". Pediatr Paring (Review). 34 (7): 485–8. PMID 23265166.
- ^ Giuca MR, Cei G, Gigli F, Gandini P (2010). "Oral signs in the diagnosis of celiac disease: review of the literature". Minerva Stomatol (Review). 59 (1–ii): 33–43. PMID 20212408.
- ^ Syphilis: Complications, Mayo Clinic.
- ^ "Loss of Tooth Structure", American Dental Hygiene Association.
- ^ "Abnormalities of Teeth", University of Missouri-Kansas Metropolis School of Dentistry.
- ^ Yip, KH; Smales, RJ; Kaidonis, JA (2003). "The diagnosis and control of extrinsic acid erosion of tooth substance" (PDF). General Dentistry. 51 (4): 350–3, quiz 354. PMID 15055615. Archived from the original (PDF) on September 7, 2006.
- ^ Neville 2002, p. 63
- ^ Neville 2002, p. 66
- ^ Neville 2002, p. 70
- ^ Neville 2002, p. 69
- ^ a b Neville 2002, p. 85
- ^ Tortora C, Meazzini MC, Garattini G, Brusati R (March 2008). "Prevalence of abnormalities in dental structure, position and eruption design in population of unilateral and bilateral crevice lip and palate patients". The Cleft Palate-Craniofacial Periodical. 45 (2): 154–162. doi:x.1597/06-218.1. PMID 18333651. S2CID 23991279.
- ^ "Dental Crowding: Causes and Treatment Options". Orthodontics Commonwealth of australia. 2020-06-29. Retrieved 2021-02-06 .
- ^ Luciane Macedo de Menezes; Susana Maria Deon Rizzatto; Fabiane Azeredo; Diogo Antunes Vargas (2010). "Characteristics and distribution of dental anomalies in a Brazilian cleft population". Revista Odonto Ciência. 25 (2): 137–141. doi:x.1590/S1980-65232010000200006.
- ^ Al Jamal GA, Hazza'a AM, Rawashdeh MA (2010). "Prevalence of dental anomalies in a population of cleft lip and palate patients". The Cleft Palate-Craniofacial Journal. 47 (four): 413–420. doi:10.1597/08-275.1. PMID 20590463. S2CID 7220626.
- ^ Amelogenesis imperfecta, Genetics Habitation Reference, a service of the U.Southward. National Library of Medicine.
- ^ Dentinogenesis imperfecta, Genetics Dwelling house Reference, a service of the U.S. National Library of Medicine.
- ^ Cho, Shiu-yin (2006). "Conservative Management of Regional Odontodysplasia: Case Report" (PDF). J Can Paring Assoc. 72 (8): 735–eight. PMID 17049109.
- ^ ASDC Journal of Dentistry for Children, Volume 48. American Society of Dentistry for Children, 1980. p. 266
Sources
- Ash, Major Thousand.; Nelson, Stanley J. (2003). Wheeler's Dental Anatomy, Physiology, and Occlusion (eighth ed.). ISBN978-0-7216-9382-eight.
- Cate, A. R. Ten (1998). Oral Histology: evolution, construction, and function (5th ed.). Mosby. ISBN978-0815129523.
- Neville, B. West.; Damm, D.; Allen, C.; Bouquot, J. (2002). Oral & Maxillofacial Pathology (2d ed.). W.B. Saunders. ISBN978-0-7216-9003-2.
- Ross, Michael H.; Kaye, Gordon I.; Pawlina, Wojciech (2002). Histology: a Text and Atlas (4th ed.). Baltimore: Lippincott Williams & Wilkins. ISBN978-0683302424.
External links
| | Await upwards tooth in Wiktionary, the free dictionary. |
- An article on the use of homo tooth used equally a neolithic pendant
- Tooth eruption chart
Source: https://en.wikipedia.org/wiki/Human_tooth
0 Response to "Does Pulling Out Your Baby Teeth Effect How Your Adult Teeth Come in"
Post a Comment